Bimonthly Internal Assessment for the month of October 2020
"This is my submission for the Bimonthly internal assessment for the month of October."
Most of the information here have been collected from different reference sites, the links to which have been mentioned. The points copy pasted have been put in quotes.
The questions to the cases being discussed can be viewed from the link below 👇
https://medicinedepartment.blogspot.com/2020/09/medicine-paper-for-october-2020-first.html?m=1
The first case presented to us is
https://swathibogari158.
57 year old man who has been an alcoholic since the past 40 years complaining of yellowish discoloration of sclera, abdominal distension & bilateral pedal edema since 3 years with a history of bilious vomitings and bleeding from gums. He also had a history of multiple blebs on his right lower limb for which debridement was done 2 years back. Patient has also been apparently taking loads of self medications over the last 4 months.Since 1 month he has been abdominal distension, Dyspnea on exertion. He also has been having reduced memory, depression & fear of dying. Over the last 5 days he has been having Multiple blebs on his left lower limb. He has also been having intermittent dark stools since the past 1 week.
Anatomical location : Liver - Acute Decompensated Liver failure
Etiological factors : Alcohol, over consumption of over the counter drugs such as NSAIDS and antibiotics.
1.Ascites is due to accumulation of fluid and salt retention along with portal hypertension.
Portal hypertension occurs due to increased hepatic resistance. Hepatic resistance occurs due to increased hepatic fibrosis as in cirrhosis and due to activation of stellate cells causing fibrogenesis. There is reduced production of endothelial nitric oxide synthase which leads to increased vasoconstriction.
There is also increased systemic circulatory nitric oxide as well as increased vascular endothelial growth factor & tumor necrosis factor that result in in splanchnic arterial vasodilation.
Splanchnic vasodilation leads to pooling of blood leads to decrease in circulating volume. This leads to compensatory vasoconstriction through the release of Antidiurectic hormone. This leads to free water retention and activation of Sympathetic nervous system and Renin angiotension aldosterone system which furthermore increases retention of renal sodium and water retention.
The information above was learnt from Harrison's Principals of internal medicine.

http://notes.medicosnotes.com/2015/04/pathophysiology-of-ascites-in-cirrhosis.html
There are two theories stated so far on the formation of Ascites :
https://www.mayoclinicproceedings.org/article/S0025-6196(11)63752-X/fulltext
1) The underfill theory
2) The overfill theory
The underfill theory states that Hypovolemia leads to stimulation of Juxtagolerular cells to release renin which releases angiotensin 1 which is converted to angiotensin 2 by ACE leading to aldosterone release from zona glomerulosa and increased retention of salt and water leading to ascites
The overfill theory states that hypervolemia along with portal hypertension results in overflow from portal system to the peritoneal cavity leading to ascites
2.Bipedal edema is due to fluid and salt retention and also due to hypoalbuminaemia. Albumin plays an important role in maintaining capillary oncotic pressure.
Reduced albumin leads to reduced capillary oncotic pressure leading to fluid leakage into the interstitial space.Further more long standing pedal edema lead to long standing venous stasis, lymphatic drainage obstruction and on top of that over the counter use of NSAIDS and corticosterioids lead to recurrent bleb formation along with ulcerations and cellulitis. Also Patients with liver failure are immunocompromised and are more prone to infections.
http://rnceus.com/lf/lfalb.html
3) Asterixis and constructional apraxia are features of Hepatic encephalopathy
Hepatic encephalopathy is a syndrome in patients with liver failure. It is characterized by neuropsychiatric abnormalities due to accumulation of neurotoxic substances in the brain.
'Ammonia is usually produced by bacteria in the gastrointestinal tract from the breakdown product of amino acids and urea followed by metabolism and clearance by the liver. In liver failure there is either a decrease in the number of functioning hepatocytes, portosystemic shunting, or both, resulting in decreased ammonia clearance and hyperammonemia.'
Once ammonia crosses the blood brain barrier, it has multiple neurotoxic effects.
These include alterations in molecular transport (e.g. amino acids, electrolytes, water) in astrocytes and neurons, increased synthesis of glutamine from glutamate by astrocytes, inhibition of excitatory and inhibitory postsynaptic potential generation, impaired amino acid metabolism, and impaired energy utilization as a result of increased GABA activity.
Asterixis is inability to maintain postural stability. Abnormal diencephalic function leads to flapping tremors when patient helds arms and wrists in extension.
Risk factors for Asterixis include Infection, GI bleed.
Usually the underlying cause needs to be addressed. Removal of ammonia by using laxatives such as lactulose and also addressing other risk factors such as infection by putting the patient on an antibiotic is required which was well addressed by the treating team.
Some of these useful points were found from the link below
https://www.unboundmedicine.com/5minute/view/5-Minute-Clinical-Consult/117471/all/Hepatic_Encephalopathy
4. Treatment efficacies
- Fluid and salt restriction along with Diuretic such as Furosemide have been advised which is addressing the fluid overload status of the patient.
- The patient has also been put on Antibiotics such as Augmentin and Metrogyl for his cellulitis. The swab culture report from the ulcer shows sensitivity to Augmentin.
- Rifaximin and Lactulose is a frequently used combination in patients with Hepatic encephalopathy.
P- 120 patients with overt Hepatic encephalopathy were randomized into two groups
I-Group A lactulose plus rifaximin 1,200 mg/day, 63 participants
Group B received lactulose plus placebo. This group had 57 participants.
C- Combination of rifaximin plus lactulose was found to be more effective than lactulose alone
O - 48 patients in group A compared to 29 patients in group B had complete reversal of hepatic encephalopathy. Reduced mortality in group A vs Group B - 23.8% vs. 49.1%. There were more deaths in group B because of sepsis compared to group A - 7 deaths in group A and 17 in group B. And patients on lactulose plus rifaximin had shorter hospital stay. There were no differences noted in GI bleed or hepatorenal syndrome.
4) Syrup Hepamerz consists of L-ornithine, L- aspartate. This reduces the accumulation of ammonia.
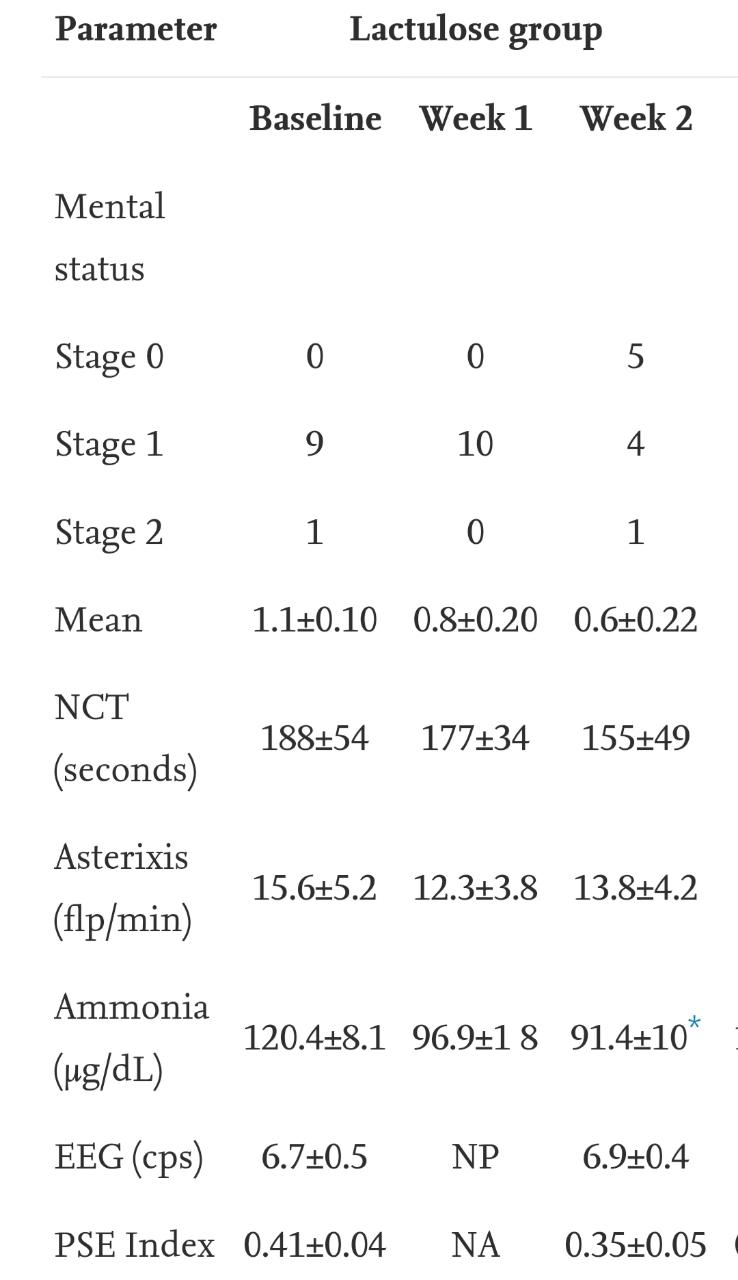
This is a randomized prospective controlled trial carried out from May 2004 to February 2006 at Mexico city comparing L- ornithine L Aspartate to lactulose
https://www.sciencedirect.com/science/article/pii/S1665268119319891
P- 20 participants with cirrhosis were included in this study.
I- 10 received LOLA at a dosage of 9grams for 2 weeks ( 1 sachet containing 3 grams for 3 times a day) where as the other 10 participants received lactulose at a dosage of 30 ml per day for 2 weeks ( syrup containing 67 grams lactulose/100ml)
C- LOLA was found to be more effective in reducing hyperammonemic hepatic encephalopathy in Mexican patients with cirrhosis
O - They were compared on the basis of mental state, number connection test, blood ammonia levels,asterixis, portal systemic encephalopathy index, EEGs, Quality of life assessment & GI side effects.



Another Randomised control placebo controlled study on LOLA
https://pubmed.ncbi.nlm.nih.gov/18983791/
P - 80 cirrhotic patients were enrolled in this study.
I- 80 patients were divided into two groups. One receiving 20g/day L-ornithine L aspartate and other receiving placebo. Both dissolved in 250ml of 55 dextrose and infused intravenously for 4 hours a day for 5 days along with 0.5g/kg of dietary protein intake everyday
C- LOLA infusions were found to be more effective in cirrhotic patients.
O- Greater improved in mental status, blood ammonia levels were noticed in participants receving LOLA.
5) Udiliv contains ursodeoxycholic acid which has shown to reduce biochemical markers of cholestasis and hepatocellular damge in patients with chronic liver disease.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1379051/
Protein powder is needed since the patient has significant hypoalbuminaemia.
7) And also the Patient should've been started on a non selective beta blocker such a Carvedilol would have been effective in preventing recurrent epsiodes of GI bleed

On admission he had anemia with leukocytosis, lft was deranged with hypoalbuminaemia (1.6 gm/dl) and deranged coagulation profile.His CT abdomen showed reduced diameters of intra hepatic portion of IVC and hepatic vein and enlarged liver. SAAG is above 1.1 mg/dl (1.2mg/dl) - could be due to portal vein thrombosis, Budd Chiari syndrome, Alcoholic hepatitis, Cirrhosis.
He was on ATT - on a combination therapy of rifampicin, INH, pyrazinamide and Ethambutol. Among which isoniazid, rifampicin and pyrazinamide are known to cause hepatotoxicity and would've further worsened the patients condition.

2. Given the patients history of prolonged nocturnal fever with sweats, dry cough, generalized weakness and weight loss along with sputum positive for Tuberculosis confirm pulmonary tb in him. His chect Xray PA view also shows
3. The ascites is because of Chronic liver failure. Because of narrowing of vessels in the portal system causing portal hypertension along with hypoalbuminaemia and fluid and salt retention as earlier explained due to activation of sympathetic nervous system.
All of these three drugs are metabolized by the liver. With the patient having Chronic liver disease there would be further more accumulation of these three drugs in the blood leading to furthermore side effects of these drugs and also more detoriation of the liver status.
Guidelines for reintiating ATT were given by American thoracic society and British Thoracic society.
https://www.thoracic.org/statements/resources/tb-opi/hepatotoxicity-of-antituberculosis-therapy.pdf
'ACCORDING TO ATS - Treatment should be interrupted and, generally, a modified or alternative regimen used for those with ALT elevation more than three times the upper limit of normal (ULN) in the presence of hepatitis symptoms and/or jaundice, or five times the ULN in the absence of symptoms.'
https://www.researchgate.net/publication/41434496_Safety_of_3_Different_Reintroduction_Regimens_of_Antituberculosis_Drugs_after_Development_of_Antituberculosis_Treatment-Induced_Hepatotoxicity
Here's an interesting case of a 22 year old man with pulmonary Kochs and Inferior vena cava thrombosis.
http://www.anncaserep.com/full-text/accr-v3-id1534.php
'Tuberculosis has several mechanisms that induce a hypercoagulable state and can lead thromboembolic complications. Hypercoagulability in tuberculosis is attributed to decreased antithrombin 3 and protein C, elevated plasma fibrinogen level, increased platelet aggregation and reactive thrombocytosis. Antiphospholipid antibody levels are high in patient with tuberculosis, deficiency of protein S have also been mentioned. '
Certain studies showed that local thrombosis is associated with increased levels of type 1 plasminogen activator inhibitor and tissue factor. Link to the point above have been taken from the links below.
https://pubmed.ncbi.nlm.nih.gov/17473582/
https://pubmed.ncbi.nlm.nih.gov/8617488/
3) The efficacy of lactulose in chronic liver failure by preventing accumulation of ammonia has already been discussed in the first case.
4) Protein powder is needed since the patient has significant hypoalbuminaemia.
5) I don't see the need for Piperacillin injections and nebulisation here. Instead the patient should've been started on second line ATT. And TIPS or liver transplant is further going to help the patient.
3rd case
https://sushma29.blogspot.com/
46 year old man with the complains of bilateral pedal edema since 1 year and abdominal distention since 1 month with a significant proteinuria >2.5 g/day

Nephrotic syndrome:
1) fluid restriction <1l/day along with salt restriction <2g/day
2) And the patients are started on diuretics.
3) Anticoagulants if needed
Furthermore the patient on corticosteriods and Immunosuppresants though their efficacy has not been significantly proven yet.
The last to go option would be renal transplant could be through a live organ donar or through Jeevandhan program.
Renal biopsy helps in diagnosing the cause of the nephrotic syndrome
2) The pros of renal biopsy would be
1.Getting to know the cause of nephrotic synrome
2. It would help us decide the treatment plan
3. Prognosis could be assessed
3) Cons of renal biopsy :
1. Bleeding is a common cause that occurs after renal biopsy
2. Infections
Renal biopsy wouldn't really put him on the road to recovery. Eventually no matter what the cause is the patient would be put either on steriods alone or on a combination of steroids & Immunosuppressants.
Here's a randomized controlled trial on cyclophosphamide and steroids in patients with idiopathic membranous nephropathy
https://jasn.asnjournals.org/content/18/6/1899
P- A total of 104 patients were recruited from March 1993 to February 1995: 53 patients in group 1 and 51 in group 2.
I - Patients were divided into two groups.
Group 1 received supportive therapy that consisted of dietary sodium restriction, diuretics, and antihypertensive agents.
Group 2 received a 6months course of alternate months of steroid and cyclophosphamide.
The treatment regimen consisted of intravenous methylprednisolone 1 g/d for 3 consecutive days followed by oral prednisolone 0.5 mg/kg per d for 27 days in the 1st, 3rd, and 5th months and oral cyclophosphamide at 2 mg/kg per d in the 2nd, 4th, and 6th months.
'Follow-up visits were scheduled every 2 weeks for 2 months, every month for 6 months, and thereafter every 6 months or more frequently when required. Parameters monitored included 24-h urinary protein and serum creatinine at each visit and serum albumin, cholesterol, and hemoglobin every 6 months.'
C - Treatment with a 6-mo regimen of cyclophosphamide and steroids induces remissions in a high proportion and arrests progression of renal insufficiency
O -


'Kaplan-Meier plots showing probabilities of dialysis-free survival (A), survival without reaching either end point (B), complete remission (C), and complete or partial remission (D). Solid line, group 1; dashed line, group 2.'



Comments
Post a Comment